
Seattle, Washington was ground zero for Covid-19 in the US and most cases in Washington State (see image below) were known to be associated with long term care homes from the very beginning. This has turned out to be true virtually everywhere in the world. This means the risk of this coronavirus to the general population is even smaller than has been assumed by health advisors. However, because numbers of care home deaths and confirmed cases are inconsistently reported worldwide, governments almost everywhere have been reluctant to lift restrictions on movements of people who do not live or work in these well-defined hotspots of Covid-19 infection.
I live in Victoria and travel to Seattle fairly often, in part because the cheapest and fastest way to Alaska and the rest of the US is via Seattle. Because of its physical proximity, I have kept a close eye on the virus situation in Seattle. In addition, a good friend of mine in Victoria had a relative in the Kirkland Life Care Centre in Seattle, which recorded one of the first deaths in the US. His ‘insider’ information tells us some interesting things about why long-term care facilities like these are being hit so hard by Covid-19. I thought it might be worth sharing what I’ve learned about this developing story.
UPDATE 25 April 2020: US Medicaid officials have summarized (as of April 23) Covid-19 deaths and confirmed cases in long term care facilities (by state) for those that report this data. They point out that until April 19, long term care homes were not required to report cases or deaths to the CDC and state [my bold]:
Our data collection effort finds that in the 23 states that publicly report death data as of April 23, 2020, there have been over 10,000 reported deaths due to COVID-19 in long-term care facilities (including residents and staff), representing 27% of deaths due to COVID-19 in those states. Our data also finds that there have been over 50,000 reported cases, accounting for 11% of coronavirus cases in 29 states. In six states reporting data, deaths in long-term care facilities account for over 50% of all COVID-19 deaths (Delaware, Massachusetts, Oregon, Pennsylvania, Colorado, and Utah; Table 2)…The total cases and deaths from reporting states accounts for just over half (53%) of all cases, and 81% of all deaths. Given that not all states are reporting data yet and the continual lag in testing, the counts of cases and deaths are an undercount of the true number of cases and deaths in long-term care facilities.
Also, the State of Massachusetts is one of those that do report long-term care facility deaths and associated cases, pdf here for April 24.
Seattle and the US

The story of ‘patient zero’ in Seattle in late January and its spread to a nearby nursing home which began the US epidemic is one many people may have missed. Here is a short synopsis taken from a National Review article (24 March 2020), How a Washington State Nursing Home Became the Center of the COVID-19 Pandemic [note the Life Care Center in Kirkland, a suburb east of Seattle, houses elderly residents but also provides follow-up care for residents of other area care homes who have had recent surgery or treatments in hospital; the bold added below is mine]:
It all began with patient zero. The 35-year-old had just returned to Seattle on January 15 from visiting family in Wuhan, China. Maybe he sneezed or coughed as he took a shared shuttle home from Seattle-Tacoma International Airport. All we know is, four days later, after feeling a little under the weather, he was in an urgent-care clinic getting blood drawn and taking throat and nasal swabs. The next day [January 19] he was confirmed as the first case of COVID-19 in the United States.
County health officials reportedly quarantined more than 60 people whom patient zero had come in contact with over those crucial four days after he returned from China. None were confirmed to have the virus. But just a few days later, it became clear the authorities had missed someone.
Firefighters soon began receiving calls from the Life Care Center, a 25-mile drive from where patient zero was being held in quarantine, at an alarming rate. Residents were reporting shortness of breath and fevers; facility staff were telling firefighters and visitors alike of an unidentified “respiratory virus.”
Life Care made 30 calls to 911 in February, up from seven the month before, but life went on at the facility as usual for its 120 residents and 180 staff. Visitors came and went, and patients were routinely discharged or moved to other nursing facilities.
As priests moved through the Life Care Center on February 26, dabbing smudges of ash on foreheads for Ash Wednesday, the virus was sweeping through as well. Patients had been getting sick for more than a week at this point, perhaps even as long as a month.
Anyone visiting Life Care could tell something was wrong. Loved ones were reaching out to the Seattle and King County Public Health Department demanding an investigation; according to an account in the Los Angeles Times, officials there “seemed uninterested.” Staff were “swamped with paperwork from government agencies,” rather than being given the help they desperately needed.
Four residents of the Life Care Center had died by the time county officials went public with the news on February 29 that more than 50 individuals associated with the center were being tested for possible coronavirus infection. Twenty-five firefighters who had responded to medical calls at the facility were placed in quarantine, and six of their colleagues later followed suit.
But it was all too little, too late: Nursing centers throughout the Seattle area began reporting cases of COVID-19. The virus soon spread all the way to North Carolina, where a resident who’d visited Life Care Center became the state’s first confirmed case.
The comment in the above quote from the National Review piece about a visitor to the Kirkland Life Care Center spreading the virus to North Carolina is an example of one of the ways the virus has spread around the city and outside the state from outbreaks in care homes. Another is the practice of low-paid care staff who work at more than one care home a day or work at a care home and another job, which is almost certainly how the illness came into the Life Care Center in the first place and then spread to others.
A good friend of mine in Victoria with whom I have daily contact, who I’ll call Carl, gave frequent updates in early March of his family’s experience with the Life Care Center epidemic. Carl had no direct contact with his family during this time but talked with them by phone.
Apparently, Carl’s sister-in-law Mary (also not her real name, in her early 60s) had been making daily visits to the Life Care Center in late February to see her 90 year old mother Dorothy, who had been sent there to recover from surgery. Dorothy was healthy enough for major surgery and normally lived at another area old age home. Mary told Carl that the other woman in the room with Dorothy had a horrible cough throughout the time she made daily visits [like hospitals, shared rooms are the norm in these facilities, sometimes four to a room].
It is unclear whether Mary’s visits stopped after 29 February when the first deaths were reported. However, on Thursday March 5, Mary was advised to self-quarantine along with her husband David. Mary had tested positive for the virus, as had her mother Dorothy, who by that time was in intensive care and not expected to survive.
By March 8, Dorothy had died of the virus. By March 10, her daughter Mary was admitted to hospital with dangerously low oxygen levels but recovered after a week or so. Husband David (Carl’s brother, also in his 60s) came down with a mild case of the virus on the 14th day of his quarantine but recovered without hospitalization. David worried that he might have passed the illness along to his own elderly parents (in their 90s) when he’d visited them a few days before he’d been quarantined but luckily, he had not.
To sum up: Ninety year old Dorothy was exposed continuously to high doses of virus from her sick roommate, all day and all night, and died quickly despite hospital treatment. Her daughter Mary was exposed to high doses of the virus during her daily one-to-two hour visits to Dorothy, developed a moderately severe illness but recovered quickly in hospital. Mary’s husband David, who had been exposed continuously to Mary both before and after Mary showed symptoms, developed only a mild case of the illness and recovered without incident at home. David did not pass the virus along during a single visit to his elderly parents before he knew he might be infected, unless they had it without symptoms (since it appears they were not tested).
This means that even though Mary had a relatively severe case of the illness that killed her mother (and presumably her mother’s roommate), her husband was only mildly ill. Although both Mary and Dorothy did not have any known underlying health conditions, it is possible both of them had emergent issues that were not severe enough to have been diagnosed but which still made them vulnerable to Covid-19. Such individual variation in undiagnosed health issues is almost never mentioned in discussions of this illness in otherwise ‘healthy’ individuals, especially patients under 70 like Mary.
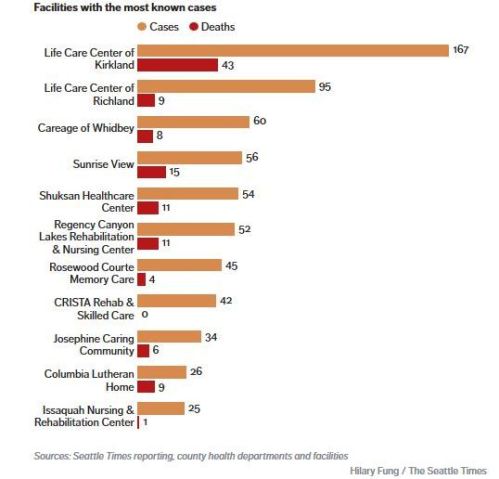
Dorothy’s continuous close contact with a coughing victim, in addition to her advanced age and weakend condition after surgery, made it almost inevitable that she would contract and then die from the illness, whether she had an unknown health condition or not. In Canada, as in the US and all European countries, long-term care facilities account for up to 50% (and sometimes more) of Covid-19 related deaths – and data from Washington State suggests that these care homes account for an even higher percentage of confirmed cases. Here is a chart of care home deaths vs. confirmed cases for the state of Washington (where tracking and testing have been better than most but still far from perfect) compiled by the Seattle Times based on data available on April 17th:
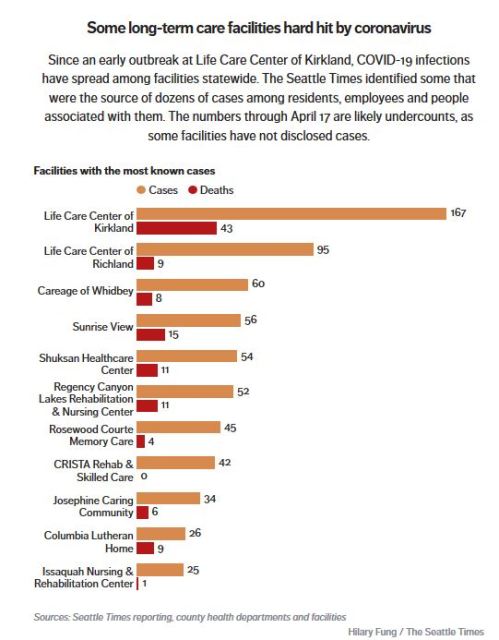
In Washington State as of April 20, the region with the highest number of cases and deaths was King County (which includes all of Seattle and where the Kirkland Life Care Center is located), with 373 deaths and 5360 confirmed cases. If the ratio of deaths:confirmed cases at the Kirkland Life Care Center (1:3.9) shown in the chart above is applied to the King County data, then 2090 plus 373 cases (2836) – 53% of the total of confirmed cases and deaths – were likely associated with long term care homes, possibly even more.
Deaths in US care homes, at April 23, surpassed 11,000 out of 46,785 total US deaths, and the data from the Kirkland Life Care Center in Seattle suggests about 4 times that many confirmed cases of Covid-19 – and possibly many more – are linked to such facilities. Therefore, more than 50% of all known cases in the US (and possibly many more in some places) are associated with long term care facilities.
Victoria and Canada
That leads me to what’s happened in Victoria (and Canada in general). Ferry traffic between Victoria and Seattle was cancelled on March 17 and the border between Canada and the US was closed to non-essential traffic on Friday March 20. Prince Harry and his family, who had moved to a suburb of Victoria in early February, took a private plane to LA just before the border closed. And even though I anticipated that Victoria might get hit hard by the coronavirus because of its proximity to Seattle and regular movement between the two cities, it apparently did not.
However, what has been surprising and frustrating to me and others, the kind of data available for Seattle is simply not available for Victoria. The BC government only reports data for ‘health regions’, which lumps Vancouver Island with a portion of the mainland north of Vancouver, which means the data provided are not even applicable to Vancouver Island as a geographic entity. The provincial authorities early on defended their decision that citizens should not know exactly where confirmed cases are located – if people knew how few cases there were in many areas, it would be impossible to enforce the province-wide lockdown – and the media have been ineffective in pressing them to change this policy.

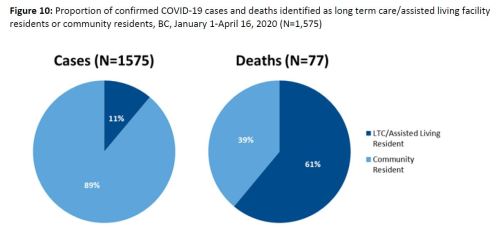
In contrast to the Washington State data shown above, which showed many more cases in care homes vs. deaths due to Covid-19, at April 16, BCCDC reported care homes had 61% of all deaths but only 11% of all confirmed cases (below). This figure has not been updated in subsequent reports. I suspect the data may not be reliable anyway because of a lack of testing and haphazard tracking.
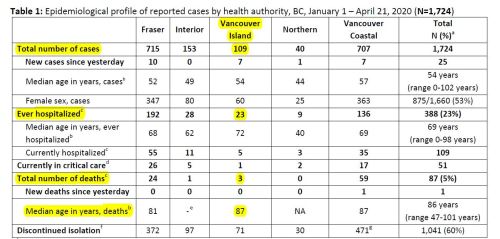
As of April 21, the most detailed daily data reported for Vancouver Island and the rest of the province appears in the table copied below, which does not include a break-down of long term care home cases or deaths. However, since the medial age of the three deaths (yes, only three) reported for Vancouver Island (87 years old) suggests that most or all of the deaths were associated with care homes. It is not clear if the authorities are even collecting data on cases associated with care homes or if they are simply not reporting them.
The lack of transparency regarding how many cases and deaths are associated with long-term care facilities skews the public’s perception of the real risk presented to the general population by this virus. A recent ‘spike’ in cases has been interpreted as a real increase in the spread of the illness that requires doubling down on lockdown measures, even though most of these are likely associated with long term care facilities and hospitalizations (ie. severe cases) overall are declining [my bold]:
This [spike in cases] tells us we have more work to do to break the chains of transmission in our communities,” said Dr. Bonnie Henry, B.C’s provincial health officer. Henry says she understands people are tired of staying at home but without a decline in cases and outbreaks it won’t be possible to ease restrictions.
“We can’t afford to have any weaknesses in our firewall if we are going to be able to move ahead in to our new normal,” she said.
Henry once again urged people to stay home if they’re not feeling well “with no exception right now.” She said that includes whether you’re experiencing mild symptoms or even if you think it’s just allergies.
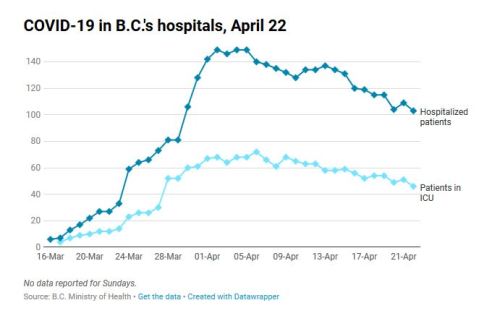
Hospitalizations at April 22 in British Columbia (below):
Statistics provided for Canada as a whole are just as lacking in transparency regarding what is happening in long term care homes. Federal health authorities only report that 18% of confirmed cases (2,538 out of 14,320) have been hospitalized and admit that 95% of deaths occurred among those aged ≥ 60 years. This suggests that overall deaths in Canada associated with long term care facilities may be 70% or more, as discussed below for the situation in Quebec and Ontario, and the data from the Kirkland Life Care Center in Seattle suggests the number of all confirmed cases associated with care homes is almost certainly much higher.
Quebec and Ontario

Two of the most populous provinces in the country, Ontario and Quebec (see map above), have been more forthcoming with their data than either BC or the federal government. Horrendous outbreaks in care homes in these two eastern provinces have been reported: as of 22 April, Quebec reported more than 80% of 1134 deaths, up from 45% in early April, were in long term care homes and Ontario reported almost 70% of 659 deaths were from such facilities. The situation is so bad in these two provinces that the federal government has promised military aid. We only know about the situation because Ontario and Quebec health officials have been reporting and discussing these care home figures all along: British Columbia and federal health officials have not.
As one Canadian editorial published today put it, “Nursing homes are COVID-19’s epicentre“. Another said, “The COVID-19 nursing home crisis wasn’t ‘unimaginable.’ It was predicted, then ignored.” Some of the media is now catching on that this is the big story of Covid-19 in the US, Canada and the UK, but the fact remains that the same pattern emerged in Europe weeks ago, with particularly horrific cases in Italy. In many places around the world (or even most), deaths in care home and confirmed cases associated with them are under-reported.
Conclusion
Media outlets and health authorities that continue to sensationalize the total number of deaths from Covid-19 without mentioning how many of these deaths are of people confined to long term care homes – Coronavirus has now killed over 50,000 people in the U.S. – are misleading the public. Including long-term care home deaths and associated confirmed cases in much-publicized overall totals tell us virtually nothing about how the virus is affecting communities at large. In short, long term care homes worldwide are the epicenter of Covid-19 and the majority of people in all communities that live and work outside such facilities have little risk of dying from Covid-19.
I have concluded from the evidence that for the general population, Covid-19 will be like a bad flu that hits a few people very hard, especially the elderly – some of whom will need hospitalization and a few with diagnosed or undiagnosed underlying health conditions will die, as happens every year with seasonal flu.
From what I have seen, there is little scientific evidence to support a continued lockdown of entire populations: the focus should be on effectively isolating and treating affected patients in long term care homes and properly tracking contacts of staff members infected with the virus, as well as isolating as much as possible people with known health conditions and those over 80 that do not live in care homes. Obviously, developing more treatment options for folks with severe symptoms would be very useful but it is unlikely that an effective vaccine is on the horizon any time soon, if ever.
Indigenous communities in the Canadian Arctic (Yukon, Northwest Territories, and Nunavut) may be almost as vulnerable to Covid-19 as those in long term care homes because so many have underlying health conditions and live in over-crowded housing. So far, the North has seen few cases, in part because there are few visitors from the south during the winter. Scientists, including polar bear researchers, have already been locked out of the Arctic in Canada and other countries for spring and summer field work, which is likely to continue into the fall.
Do we need a continued enforcement of ‘social distancing’ and bans on group events? Should everyone be wearing masks? Journalist Jonathan Kay has written up a thought-provoking analysis of Covid-19 ‘super spreader events‘ (‘SSE’, 23 April 2020: COVID-19 Superspreader Events in 28 Countries: Critical Patterns and Lessons) that’s a must-read. He concludes [my bold]:
When do COVID-19 SSEs happen? Based on the list I’ve assembled, the short answer is: Wherever and whenever people are up in each other’s faces, laughing, shouting, cheering, sobbing, singing, greeting, and praying.
Even still, Kay (like virtually all others), does not consider the probability that some people (even children and infants) can have underlying health issues that have not been severe enough to generate a diagnosis but which still make them vulnerable to developing a severe or even fatal case of Covid-19 (or even seasonal flu). The fact that not every apparently ‘healthy’ person under 80 is equally vulnerable means that even in the ‘super spreader events’ Kay examined, only a few of those infected became severely ill and even fewer died.
All of this confirms my impression that forcing people to line up at banks, grocery stores and pharmacies so that only a limited number of people are in a building at the same time (and then forcing them to shop in one direction only to maintain a distance of 2 metres apart), keeping healthy children out of school and forbidding them from playing with friends, and prohibiting almost everyone from working is doing virtually nothing to limit the spread of deadly cases and is frightening people unnecessarily.
Like many others, I have lost my job because of this lockdown. University classes were cancelled on March 16 and all ‘non-essential’ research on the University of Victoria campus was forbidden on March 26. This decision to lock out researchers – which appears to have been made by the university, not mandated by the government – put me out of work. University professors are still being paid, as are administrators, and the university is still collecting tuition fees from students. Teaching will be provided remotely until at least September, which means there is little incentive for the university to allow me back to work before then.
The way I see it, daily figures reported by health authorities for deaths and confirmed cases need to be presented both ‘with’ and ‘without’ numbers associated with long term care homes and similar facilities. Until then, the government’s overcautious response is unlikely to change and the publics’ unrealistic fear that Covid-19 is everywhere just waiting to kill them is unlikely to be relieved.



You must be logged in to post a comment.